| Reference | 1. Drugs. 1995 Apr;49(4):563-76. <br />
Trimetrexate. A review of its pharmacodynamic and pharmacokinetic properties and
therapeutic potential in the treatment of Pneumocystis carinii pneumonia. <br />
Fulton B(1), Wagstaff AJ, McTavish D. <br />
Author information: <br />
(1)Adis International Limited, Auckland, New Zealand. <br />
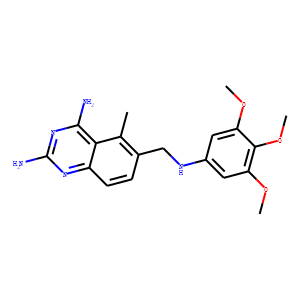
Trimetrexate is a folinic acid analogue structurally related to methotrexate,
whose primary mechanism of action is believed to be inhibition of dihydrofolate
reductase. This reduces the production of DNA and RNA precursors and leads to
cell death. Trimetrexate is lipophilic and can passively diffuse across cell
membranes including those of Pneumocystis carinii and its mammalian host. To
minimise toxicity, trimetrexate must be coadministered with calcium folinate
(leucovorin calcium), a reduced folate coenzyme, which is transported into, and
protects, mammalian host cells but not P. carinii cells. In noncomparative trials
trimetrexate was effective in the treatment of P. carinii pneumonia (PCP) in
patients with AIDS who were intolerant of or refractory to cotrimoxazole
(trimethoprim/sulfamethoxazole) and pentamidine treatment. In these patients, 2-
to 4-week survival rates of 48 to 69% were reported. In a comparative trial in
the initial therapy of PCP, trimetrexate was less effective than cotrimoxazole in
moderate to severe disease as evidenced by a significantly higher failure rate.
Trimetrexate was better tolerated than cotrimoxazole when used in this setting,
however. Significantly fewer patients receiving trimetrexate plus calcium
folinate discontinued treatment because of adverse events than did patients
receiving cotrimoxazole. The most common adverse effect associated with
trimetrexate is myelosuppression (neutropenia and thrombocytopenia); this is
mitigated by coadministration of calcium folinate and is generally reversible
upon dosage reduction or discontinuation. Other adverse effects include increases
in serum aminotransferase levels, anaemia, fever, rash/pruritus, and increased
alkaline phosphatase or serum creatinine levels. Further research into the use of
trimetrexate, including its efficacy as prophylaxis, in combination with other
agents and as an oral formulation, is needed to clearly define its role in the
treatment of PCP and to identify patients most likely to benefit. Currently,
trimetrexate should be considered as an alternative treatment option in
immunocompromised patients with moderate to severe PCP who have not responded to
or are intolerant of first-line therapy. <br />
2. Ann Pharmacother. 1992 Feb;26(2):218-26. <br />
Trimetrexate for Pneumocystis carinii pneumonia in patients with AIDS. <br />
Amsden GW(1), Kowalsky SF, Morse GD. <br />
Author information: <br />
(1)Clinical Pharmacokinetics Laboratory, Millard Fillmore Hospital, Buffalo, NY
14209. <br />
OBJECTIVE: The primary objective of this article is to introduce readers to the
use of a new agent, trimetrexate (TMTX), in the treatment of Pneumocystis carinii
pneumonia (PCP). The article also gives the readers an overview of PCP and
discusses some of the controversies surrounding it. Pharmacokinetic data and
clinical trials are reviewed, as well as adverse effects, drug interactions, and
dosage guidelines.<br />
DATA SOURCES: A MEDLINE search was used to identify pertinent literature,
including reviews.<br />
STUDY SELECTION: As both pharmacokinetic and clinical trials were few in number,
all available trials were reviewed.<br />
DATA EXTRACTION: Pharmacokinetic data from trials involving patients with AIDS
was sparse; therefore, those involving oncology patients, including a pediatric
population, were included. Although more trials need to be done in AIDS patients,
the results from the oncologic trials give us a baseline from which to
extrapolate. All clinical trials available at the time of publication were
reviewed as were all of the preliminary results from three ongoing trials, which
were made available through a personal communication.<br />
DATA SYNTHESIS: TMTX has been found to be 1500 times more potent than
trimethoprim as a dihydrofolate reductase inhibitor, and has the potential to
provide an effective therapeutic option for PCP. TMTX is a lipid-soluble analog
of methotrexate and is thus capable of greater penetration into Pneumocystis
cells, which lack the folate membrane transport system necessary to take up
classic folate structures like leucovorin and methotrexate, thereby negating any
clinical effectiveness of methotrexate and allowing leucovorin to be used for
host cell rescue. TMTX/’s pharmacokinetic parameters best fit a multicompartmental
model with a terminal half-life of up to 12 hours. It is cleared both hepatically
and renally with up to 41 percent excreted unchanged in the urine. Although
TMTX/’s pharmacokinetic parameters are variable, the need for plasma concentration
monitoring at present is unclear, as no dose-response relationship has been
established. <br />
3. J Clin Oncol. 1987 Dec;5(12):2032-40. <br />
Trimetrexate: a second generation folate antagonist in clinical trial. <br />
Lin JT(1), Bertino JR. <br />
Author information: <br />
(1)Department of Medicine, Yale University School of Medicine, New Haven, CT. <br />
Trimetrexate is a promising new lipophilic antifolate with antitumor and
antimicrobial activity, which is currently undergoing clinical trials. It differs
from methotrexate in its transport and intracellular retention, and may be useful
against tumors resistant to methotrexate because of impaired transport or
deficient polyglutamylation. In preclinical studies, it has demonstrated a
broader spectrum of antitumor activity than methotrexate, and appears to have
synergistic antitumor activity when combined with a number of other agents. In
clinical trials, the primary toxicity has been hematologic, with rapid recovery
and no evidence of cumulative dose effect. Nonhematologic toxicity has been
sporadic. Preliminary results of phase II trials indicate activity against
breast, non-small-cell lung, and head and neck tumors. In addition, trimetrexate
with simultaneous leucovorin rescue appears to be a promising new treatment for
pneumocystis pneumonia in AIDS patients, with minimal toxic side effects. <br />
|